Embryology Questions Medical School -
Eine erschwingliche Hochleistungs-FEM-Lösung.

Eine erschwingliche Hochleistungs-FEM-Lösung.
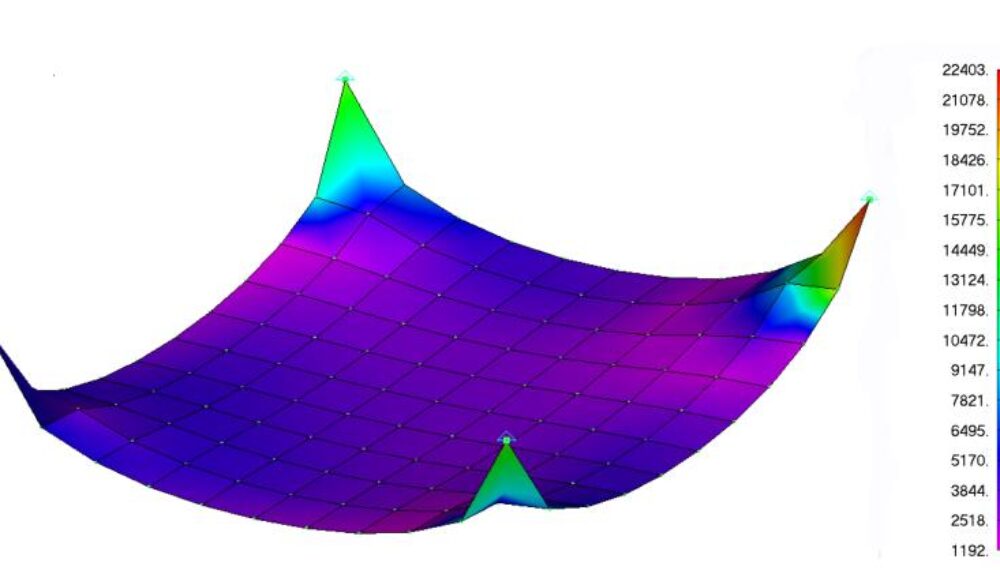
Simcenter Femap ist Teil des Siemens Digital Industries Software Simcenter Produktportfolios und eine der bekanntesten FEM-Lösungen. Simcenter Femap wird in der Branche seit über 30 Jahren angewendet. Mit dem Programm bereiten Sie Ihre Simulationsmodelle vor (Pre-Process) und erhalten eine umfassende Darstellung der Analyseergebnisse (Post-Process). Die Software ist offen für alle kommerziellen Solver, darunter Simcenter Nastran, Ansys, LS-DYNA und Abaqus und kann auf Geometriedaten aller großen CAD-Systeme zugreifen.
Von Anfänger bis Fortgeschrittenen kombiniert Simcenter Femap außergewöhnliche Benutzerfreundlichkeit mit Kosteneffizienz und hat das Potenzial, die anspruchsvollsten Probleme zu modellieren.
Prospekt
Für Simcenter Femap gibt es mehrere Möglichkeiten, die Lizenz zu erwerben:
Neben der Basisplattform stehen mehrere Zusatzmodule zur Verfügung, die auf die gleiche Weise flexibel ergänzt werden können. Auch hier ist es möglich, die Module über Token einzustellen. Möchten Sie mehr wissen?
Femap kostenlos testen Mietlizenz
Online Angebot Studentenlizenz
Als Referenz haben wir eine Reihe von Femap Fallstudien für Sie pro Industrie gruppiert.
Als Teil des Simcenter Mechanical Portfolios bietet Femap die Möglichkeit, praktisch jede Art von Konstruktion oder Bauteil mit dieser Software zu modellieren und das Verhalten für jede Betriebsumgebung zu bestimmen. Die umfangreiche Solver-Unterstützung beschleunigt den Analyse- und Simulationsprozess erheblich. Das spart Ihnen Zeit und Geld. Im Ingenieurwesen beschleunigt sich das Tempo des Wandels schnell, so dass Sie eine solide, aber zukunftssichere Software wählen müssen, die echte Produktivitätsgewinne ermöglicht. Femap ist eine ausgereifte, robuste Lösung und eine solide Investition.
Bei Femto Engineering unterstützen wir Firmen dabei, ihre innovativen Projekte zu verwirklichen: mit Engineering, Training, Support, F&E und SDC Verifier.
Wir sind in den Benelux Ländern lizensierter Händler für Simcenter Femap, Simcenter Simcenter 3D, Simcenter Amesim und Simcenter STAR-CCM+. Melden Sie sich bei uns und lassen Sie die FEM und CFD Tools für sich arbeiten.
Melden Sie sich für unseren Newsletter an, um kostenlose Ressourcen, News und Updates monatlich in Ihrem Posteingang zu erhalten. Teilen Sie unser Fachwissen!
Failure of fixation → malrotation → Ladd’s bands across duodenum → duodenal obstruction + risk of midgut volvulus (twisting around SMA).
Kartagener syndrome (immotile cilia) causes situs inversus, but that's not an NTD. 2. Pharyngeal Arches – The “Cranial Nerve & Artery” Matrix The embryology: Six arches (though 5th regresses). Each arch has its own: Cartilage (bone), Nerve, Artery, Muscle.
| Condition | Defect | Phenotype | Exam clue | |-----------|--------|-----------|-----------| | | Androgen receptor defect | 46,XY; female external genitalia, blind-ending vagina, testes in abdomen/labia, no uterus, sparse pubic hair | Inguinal hernia with gonad in adolescent female. | | 5-alpha reductase deficiency | Can’t convert T→DHT | 46,XY; ambiguous genitalia at birth, virilization at puberty (penis enlarges) | “Guevedoces” (penis at 12). | | Müllerian agenesis (MRKH) | Müllerian duct failure | 46,XX; absent uterus & upper vagina, normal ovaries, normal external genitalia | Primary amenorrhea with normal secondary sex characteristics. | | Persistent Müllerian duct syndrome | No MIS or receptor defect | 46,XY; male external genitalia + uterus & fallopian tubes | Cryptorchidism + hernia with uterus. |
If you are a medical student, you have likely asked: “Why do I need to know the pharyngeal arches?” The answer lies not in memorizing diagrams, but in understanding that embryology is the logic board for adult anatomy and congenital anomalies. On exams (USMLE, COMLEX, in-house shelf exams), embryology questions are rarely pure recitation. They are clinical vignettes disguised as developmental biology. Embryology Questions Medical School
| Arch | Nerve | Muscle derivative | Cartilage derivative | Clinical correlate | |------|-------|-------------------|----------------------|--------------------| | 1 (Mandibular) | CN V3 | Muscles of mastication, mylohyoid, tensor tympani | Meckel's cartilage → mandible, malleus, incus | (arch 1 neural crest failure) – micrognathia, zygomatic hypoplasia. | | 2 (Hyoid) | CN VII | Muscles of facial expression, stapedius, stylohyoid | Reichert's cartilage → stapes, styloid process, hyoid (lesser horn) | Branchial fistula (persistent cervical sinus) – drainage from anterior border of SCM. | | 3 | CN IX | Stylopharyngeus | Hyoid (greater horn) | Isolated – rare. | | 4 & 6 | CN X (superior laryngeal & recurrent laryngeal) | Cricothyroid (4), intrinsic laryngeal muscles (6) | Thyroid, cricoid, arytenoid cartilages | DiGeorge syndrome (22q11.2 deletion) – affects arch 3, 4, 6 → thymic aplasia, cardiac outflow tract defects, hypocalcemia. |
| Mechanism | Defect | Clinical pearl | |-----------|--------|----------------| | Failure of endocardial cushion fusion (neural crest cells) | (ostium primum ASD + VSD + cleft mitral valve) | Associated with Down syndrome (40% of Down patients have AV canal). | | Abnormal conotruncal septation (neural crest migration failure) | Transposition of great arteries (TGA), Tetralogy of Fallot (TOF), Truncus arteriosus | TOF = VSD, overriding aorta, RVH, pulmonary stenosis. Boot-shaped heart. TGA = cyanosis day 1, needs prostaglandins to keep PDA open. | | Failure of spiral septum rotation | Dextro-TGA (aorta from RV, pulmonary from LV) | Incompatible with life unless mixing (ASD/VSD/PDA). | | Abnormal ductus arteriosus closure | Patent ductus arteriosus (PDA) | Machine-like murmur. Associated with rubella (also cataracts, deafness, PDA). |
Master that framework, and you will not only pass – you will outthink the question writers. Failure of fixation → malrotation → Ladd’s bands
“1st part of maxillary, 2nd stapedial + hyoid, 3rd common carotid & proximal ICA, 4th arch: left = aortic arch, right = proximal subclavian, 6th: left = ductus arteriosus, right = proximal pulmonary”
Dextrocardia (heart on right) with situs inversus is not a heart defect per se – it’s a laterality defect from ciliary dysfunction (Kartagener). Dextrocardia with situs solitus is a severe heart malformation. 4. Foregut & Midgut Rotation – The “Malrotation & Volvulus” Danger The embryology: Midgut herniates at week 6, rotates 270° counterclockwise, returns at week 10.
When you see a baby with a heart defect, think neural crest . When you see bilious vomiting, think malrotation . When you see a neck mass that moves with swallowing, think thyroglossal duct . When you see ambiguous genitalia, think androgen synthesis or action . Pharyngeal Arches – The “Cranial Nerve & Artery”
Neonate with bilious vomiting (green) → rule out malrotation until proven otherwise. Upper GI series shows “corkscrew” or “duodenal jejunal junction to the right of spine.”
Recurrent laryngeal nerve (branch of CN X, arch 6) loops under the right subclavian artery on right, ligamentum arteriosum on left. If a patient has a dysphagia lusoria (aberrant right subclavian artery), the nerve takes a direct course to the larynx – this is a known surgical variant. 3. Heart Tube Looping & Septation – The “Conotruncal” Nightmare The embryology: Heart tube forms week 3, loops to the right by day 23. Septation occurs weeks 4-7.